Life After USAID: How Will Kenya Finance... HIV Care?
All U.S. Agency for International Development (USAID) staff have been placed on administrative leave globally, in a brief message posted on the website marking the end of the agency.


All U.S. Agency for International Development (USAID) staff have been placed on administrative leave globally, in a brief message posted on the website marking the end of the agency.
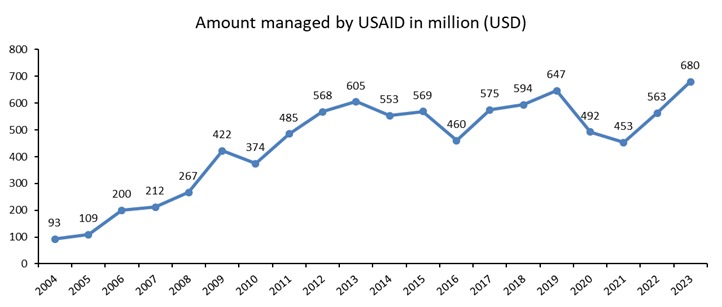
There is uproar, concern, and anxiety over the closure of development circles, like the impending shutdown of USAID. In Kenya, USAID has spent KES 772.6 billion shillings in the last two decades, from 2004 to 2023, according to Defrontera’s analysis of data from the US government's website for “making U.S. foreign assistance data available to the public.” While the country has received about KES 1.7 trillion in total from the United States at this time, the funds were primarily channelled through USAID.
Where is USAID in Kenya in 2025?
Documents that Defrontera exclusively obtained from a source close to the agency showed that the agency had various projects where money had been allocated (set aside but not disbursed) from last year to October 2025. USAID had two or three projects embedded in the counties' structures in all but one county (Tana River). HIV and related activities are in 34 counties. Global health security, which involved activities to ensure that Kenya’s health system could prevent, detect, and respond to infectious disease threats quickly, is in 26 counties.
The other areas of focus were intense support for tuberculosis in 14 counties, malaria in all the eight counties in Nyanza, and family health in nine counties. Kisumu County’s health executive, Dr Gregory Ganda, told Defrontera that the county will now have to budget for 567 healthcare providers working in health facilities who cared for the county on four USAID-supported projects. The healthcare providers care for HIV patients and others in public health facilities.
Dr Ganda has done the maths and summarised his concerns in a WhatsApp message to Defrontera: “Human resources who have salaries for January and February, serving approximately 115,000 clients across 153 sites… 4,000 men who have sex with men, 6,000 female sex workers, 600 injectors [who get care] in 9 Drop-in Centres.”
Kisumu County’s next course of action is to “close down clinics dealing with special populations and relocate them to public facilities, private facilities to bill for services, and close down clinics and reorganise the clients,” according to Dr Ganda.

Many more Kenyans have expressed concerns about how the 1,378,457 people living with HIV will not have access to life-preserving antiretroviral therapy (ART). ARVs are a combination of HIV medicines that people take daily, monthly, or every other month to stop the virus from multiplying and eventually overpowering the person’s immunity.
In 2013, 58,446 Kenyans died of AIDS—the medical term when your immunity has collapsed because the virus has colonised it. Thanks to ARVs, the deaths reduced by 64% to 20,480 in 2024, according to data from Kenya’s National Syndemic Diseases Control Council. The President’s Emergency Plan for AIDS Relief (PEPFAR) programme is Kenya’s largest source of funding for HIV care and treatment services and receives its funding from the U.S. Agency for International Development (USAID).
How many health facilities will this affect in Kenya?
It is not the lack of ARVs that has all healthcare specialists worried; they are concerned about the package of care that must accompany the ARVs for the patient to live, as seen in cases like that of Roselida Asiko. When the mother received her diagnosis, she contemplated ending her life. Her husband had died a few weeks before she learned she was HIV positive. Her father, who had lived with HIV for years, took her to Lumumba Health Centre in Kisumu County, a health facility supported by USAID.

Lauded as a model for the care of people living with HIV, Lumumba follows the national guidelines for looking after people living with HIV to the letter. We spent a day at the facility to see what care Roselida and other patients receive at Lumumba. As a regular patient, Roselida’s journey is much shorter, and the length of her stay in the facility was largely due to her conversations with the staff who have cared for her over the past nine years. When she fell pregnant, Roselida received medicine to prevent her from transmitting the virus to her unborn children. None of her two children is HIV-positive.
“They are good to me, they monitor how I am doing closely, like that time I reported rashes on my body, the doctor ran tests , and then they changed the medication I was taking, and the rashes disappeared,” Roselida told Defrontera.
When the patient comes to the facility, either through the outpatient, TB, or Mother and Child clinic, a counsellor talks to the patient, preparing them psychologically for their interaction with the health facility and assuaging the fears they may have if they turn out to be HIV positive.

After the counsellor, a clinician checks the patient’s vitals such as blood pressure, weight, and nutritional status. Another clinician tests the patient for opportunistic infections, illnesses that people with HIV fall prey to due to their compromised immune systems, such as tuberculosis, malaria, and other sexually transmitted infections. The patient is also checked for other issues, like mental illness and any signs of gender-based violence.
Peter Ogutu, the clinician in charge of Lumumba Health Centre, told Defrontera: “If the tests return a positive result, like they have TB, mental illness, or any other infection, these will have to be treated first before anything else if the patient is to have a positive outcome.”
The clinicians also check the patient’s viral load to see how much virus is in their blood, as this will determine what type of ARVs they will receive from the facility. The patient’s data is entered into an automated system that will alert the facility of missed medical appointments, and a community health assistant will be sent to trace them at home to find out where they are.
Adherence costs
Throughout the care of the patient, the clinicians at Lumumba check if the patient has developed resistance—when the medication becomes powerless against the virus—or the patient’s response. Most of the resources that pay the staff, laboratory costs, such as the equipment, reagents, and the personnel, came from PEPFAR.
It is difficult to calculate the price of looking after one HIV patient, as there are so many expenses throughout the care lifecycle, but some studies have estimated that the medicine for a patient like Roselida costs around KES 30,000 per year. As of January 2025, there are about 3,840 health facilities that offer treatment and care to HIV patients in Kenya, according to Kenya’s National AIDS and STIs Control Program (Nascop).
However, there are “adherence” costs, and this is what healthcare providers are concerned about. This is the money that goes into paying community health assistants, peer educators, and public health officers to track worn-out patients and keep them on their pills. This is old-school boots-on-the-ground healthcare, which can include tracking patients to their homes and even personally accompanying them to the healthcare facility. More than a decade ago, the adherence cost in Kenya was estimated to be KES 30,000 in health facilities that have been supported by PEPFAR to purchase medicine and pay salaries, like Lumumba Centre in Kisumu, in western Kenya.
In counties where this 360-degree care is not available, like Lamu, after PEPFAR withdrew, cases of mothers transmitting the virus to their children have been recorded. Since 1972, when USAID came to Kenya, the government of Kenya has relied on the funds they provide, especially in the 1990s when the HIV/AIDS pandemic became a huge public health crisis. Kenya has budgeted with the USAID funds in mind. Not much has changed even after the country voted to devolve healthcare services to the 47 health units in 2013. Sources in the Council of Governors, who requested not to be identified, said that in some counties, funds from the USAID account for as much as 50% of the health budget. In the last week, multiple non-profits, including the University of Nairobi, have sent letters to their staff asking them to work for three months without pay.
Share this feature


