To the locals, it is the county with a health system that cannot fully support its HIV patients.
To the world, the Lamu Archipelago is a renowned UN World Heritage site in Kenya that is a magnet for tourists. To the locals, it is the county with a health system that cannot fully support its HIV patients after a slash in funding. Now, HIV infections among adults are rising.

Whenever Dorcas Gichinga needs to get to her local hospital to collect her HIV medication, she is faced with a set of hard choices: walk for three hours from her home in Majembeni town to Mpeketoni Sub-County Hospital in the coastal county of Lamu in Kenya; walk one way for about an hour and then pay Sh400 (about $3) for the return trip in a matatu, a local bus; or take a bike—boda boda—at the cost of Sh2,000 for the trip (about $15).
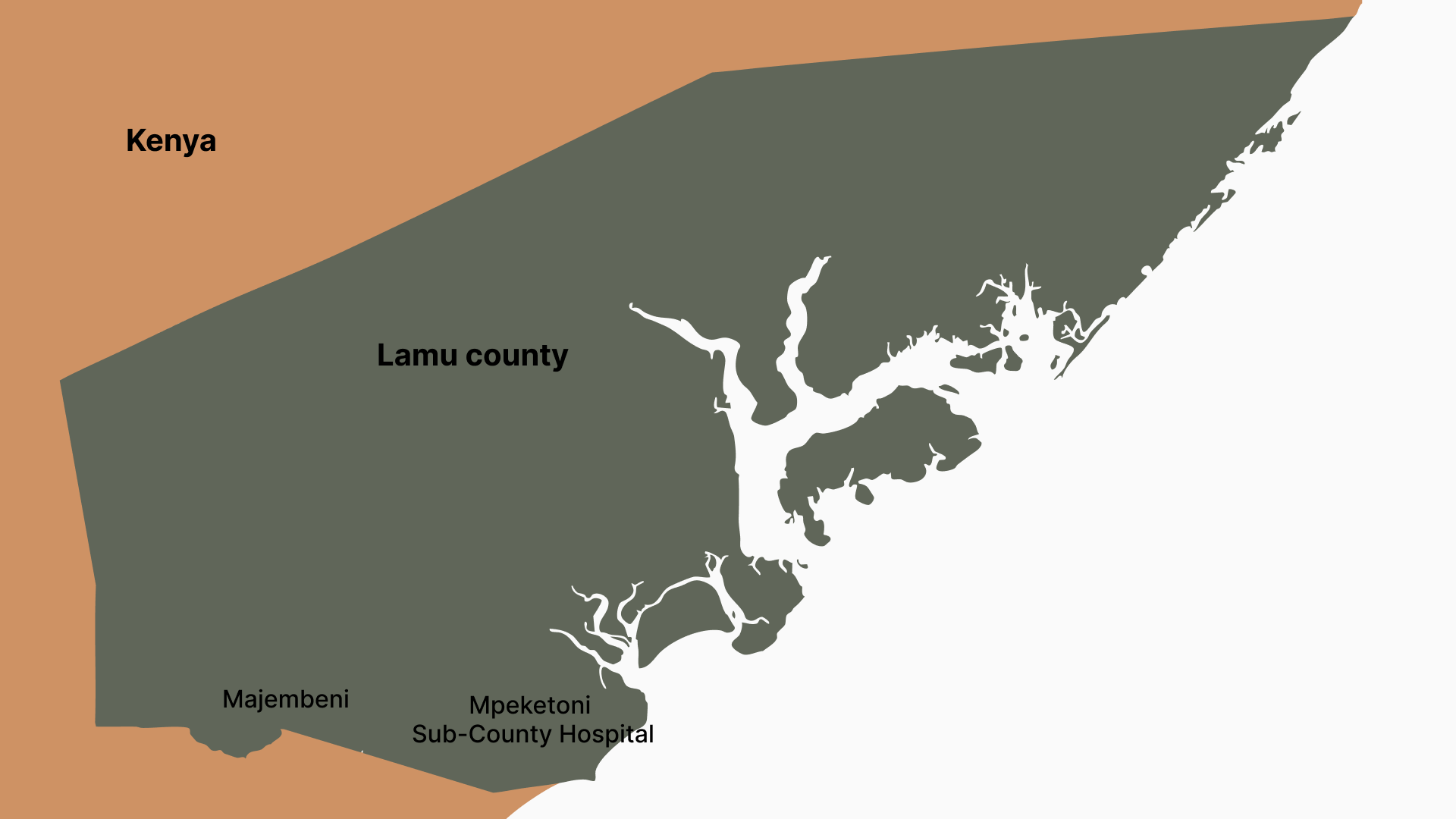
She makes these trips every month to Mpeketoni Sub-County Hospital, the nearest public health facility where she can get free HIV services, including antiretroviral drugs (ARVs). On the day she talks to us, Dorcas has borne the bristling three-hour walk, braving the melting coastal heat. She says her throat is parched and her feet ache. A subsistence farmer and casual labourer, she has to make these trips.
“I make around Sh3,000 a month. I cannot afford to pay for transport; it was either I walk or miss another month of medication,” she said.
Dorcas is one of the 2.7% of the population in Lamu County that are living with HIV. As routine care, Dorcas should get certain specific medical services, free of charge in public health facilities: she should get the ARVs, the medicine that suppresses HIV levels, prevents an infected person from transmitting the virus to another sexual partner and cuts the risk of transmission from infected pregnant women to their babies; a nutrition check-up, see a psychologist, get tests for any other infections that may take advantage of her compromised immunity, and other advanced tests to determine whether her kidneys are functioning well.

When she was diagnosed in the capital, Nairobi, she received the whole package and support to attend the facility for her medicine and tests. When she moved to Lamu, where land is affordable, the mother of two now must dig into her already stretched pocket to fund trips to the hospital and meet her daily needs.
“On clinic days in Nairobi, they would give us fare and lunch. So, it was easy for us to take the medication as scheduled, but life is so much harder in Lamu,” she said.
Dorcas’ financial circumstances mirror Lamu County’s. Her $15 income is six times lower than what other women earn (about $90), too little to provide for herself and her two children. Just as going without food has become a norm for her and her children due to her diminished fortunes, the county has had to reduce spending when the changes at the country’s biggest source of funds prioritised 40 other counties with more people living with HIV.
The President’s Emergency Plan for AIDS Relief, or PEPFAR, is a $7.5 billion programme from the United States that has delivered lifesaving treatment to more than 20 million people in Kenya and 53 other countries.
PEPFAR out; government silent
Dr Rose Nafula, the head of Kenya’s National AIDS and STIs Control Programme (NASCOP), said that from 2015, PEPFAR focused its strategy on counties with more people living with HIV. PEPFAR left out Lamu and six other counties in the arid and semi-arid region: Wajir, Mandera, Tana River, Garissa, Marsabit, and Isiolo.
Dr Wafula told Defrontera: “It is the direct facility support like paying healthcare workers, community-level coordination, and facilities utilities that were shifted from those counties and concentrated this specific support to 40 counties. However, for commodities, the support is for all counties.”
The impact of the reduced money has been swift and deadly: the number of people living with HIV has risen from 1.5% in 2022 to 2.2% presently, according to Dr Mbarak Bhajaj, Lamu County Executive Committee Member for Health. The number of patients receiving their ARVs at the county’s biggest health facility, King Fahad Referral Hospital, reduced from 420 to 404 in just a month.
Perhaps the saddest consequence of the decline in funding is the rate of transmission from HIV-positive mothers to their unborn children.
“Mother-to-child transmission in Lamu has increased from 9 to 12 per cent in the last year,”
Lamu HIV Coordinator Fatma Mohamed told Defrontera.
The number has increased because, like many infectious diseases, HIV is as much a social disease as it is viral, especially in locations like Lamu. The archipelago is Kenya’s oldest town with a rich Mediterranean-influenced conservative Swahili culture.
PEPFAR relied on numbers—a small 144,000 population, fewer people living with HIV—and so does the national government in the money it allocates to the county. This, Dr Bhajaj said, was a miscalculation with major public health implications as it ignored the social aspects of HIV.
Dr Bhajaj explained: “Lamu receives Sh3.2 billion a year, the least of all the 47 counties, and we allocate Sh1.2 billion of this to healthcare. Of this, only around Sh5 million goes to programmes focused on common illnesses such as HIV, malaria, or tuberculosis.”
Since 2003, PEPFAR has spent KES 1.0376 trillion in Kenya. The PEPFAR money has employed 43,000 healthcare workers who work in the hospitals, paid for community programmes such as peer education, and supported health workers following up on patients worn down by stigma or infections that prevent them from visiting health facilities.

Lamu elder and Muslim cleric Mohamed Abdulkadir says people in Lamu, especially the dominant Swahili and Bajuni communities, shy away from topics surrounding sex and sexually transmitted diseases. In such a conservative culture, the silence has fuelled the rising cases of sexually transmitted diseases, including HIV, as the population remains unaware of how to protect themselves from infections.
The cleric explained: “We have fewer casual sexual encounters in Lamu because we do not have nightclubs and sex workers on the streets as is the case in neighbouring Mombasa County, but Islam allows polygamy, which has added pressure on HIV infection. Having two to four wives isn't a joke. We have seen a rise in HIV infections among married people because people are not being faithful to their spouses.”
With money only available for medicine, there is hardly any follow-up, but “our geographical challenges make navigating the different islands a logistical nightmare”, Dr Bhajaj said.

Lamu is made up of around 65 islands. For instance, the cost of a 15-minute boat ride is up to Sh1,000 ($8), more than double what people typically pay for a car ride.
I’m weak; I’ve lost weight.
Religious leaders like cleric Mohamed Abdulkadir, without standardised information on what they should tell the community, have now opted to spread sexual education through mosque sermons for congregants and even other members of the public.
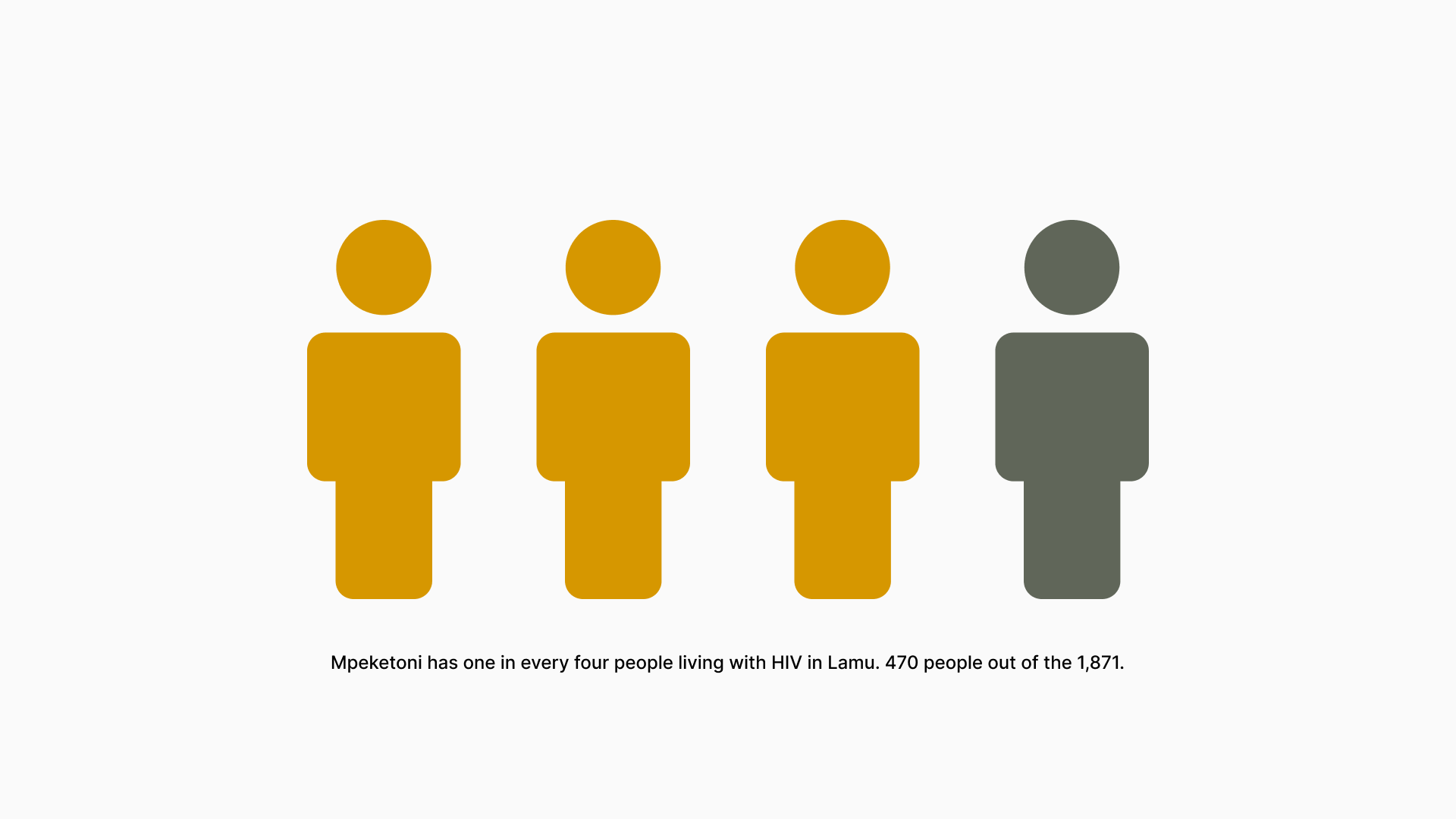
Apart from the poverty, people living with the virus can fall sick, unable to fend for themselves if they do not have support systems around them. This is more common than it is rare, especially for impoverished, dry parts of Lamu, such as Mpeketoni, a ward at the peripheries of the county. Mpeketoni has one in every four people living with HIV in Lamu—470 people out of the 1,871.
“I feel weak, I have lost weight. I know that staying without medicine is dangerous. I came to the hospital today because the doctor called me to tell me that it’s been two months since I picked up my medicine. I did not forget to come for my medicine. I wish that they could bring us the medicines like they used to,” she says.
Defaulting comes with deadlier consequences than the death of the patient.
“Anti-retroviral therapy is not only a treatment measure but also a preventive one. When patients don’t adhere to treatment, they transmit the virus more easily and the HIV burden grows,” says Lamu HIV Coordinator Fatma Mohamed.
After the departure of PEPFAR, and the silence from the national government to cater for what the donors were funding, the county has been relying on small local non-profits; three NGOs were working on health as of 2016, and they have since become fewer. Kisumu County, which has PEPFAR support and the third highest HIV prevalence in Kenya (19.3%), has 187 non-profits. The last remaining NGO—the Witu Community Development Programme (WICODEP)—ended its operations in June this year.
“With WICODEP’s end, all our community outreach efforts have ground to a halt,” reveals the county HIV Coordinator, Ms Mohamed.
Now, with no funding, community health workers have stopped transporting the drugs to villages where patients can access medication easily. Consequently, patients like Gichinga have joined the growing number of those who have defaulted from treatment—the cost of keeping up with prescriptions becoming simply too high.
Pushed into a corner, the county will use the money meant for other basic medical needs in the county.
Share this feature


