Systems, Silence, Spread: Kenya’s imminent Tuberculosis Crisis Amid Funding Cuts
As Kenya’s fight against tuberculosis unravels under drug shortages, funding cuts, and missed diagnoses, patients like Joel Owino are left vulnerable—and so are the communities around them.


Joel Owino, 52, says his body is fading away, partly due to his two-year battle with tuberculosis (TB). Mr. Owino, who was born in Simenya village in Siaya County in western Kenya, says he was first diagnosed with TB in 2023. He diligently took the medication for six months as guided by the clinicians, and he thought he had healed.
In September 2024, the disease—characterised by a persistent cough and visible weight loss—came knocking again. As was the case the first time, he visited a dispensary in Simenya, but the father of five was sent to Ambira Level 4 Hospital for another test. For a man whose body’s defence system was already strained from two other chronic conditions, another bout of TB was the last thing he needed.
"I tested positive again and was put on medication again for another six months, and I finished them on February 17, 2025," he said.
The to-do list of care that Joel has had so far—getting tested, getting medication with counselling on how to take the medicine—is part of the national guidelines that dictate how the health system handles tuberculosis patients like Joel.
The elaborate algorithm-like process skipped a step for Joel, and it has endangered his life, the children living with him, and the community around him: In his last visit, Joel did not go to Ambira or any higher-level health facility in Siaya County to take a test to confirm whether he still has tuberculosis. Had he taken this test, he would not only have known whether he had TB but also if it was the more aggressive, virulent type that does not respond to Isoniazid and Rifampicin, the first-line medication for treating TB, according to the Ministry of Health.

In Kenya, the Ministry of Health’s guidelines modelled after the World Health Organization (WHO), dictate that healthcare workers have three ways to determine whether a person has TB: by observing the physique of the patient—persistent coughing, losing weight, fever, and night chills—or a collection of sputum, which is tested in a lab through growing the bacteria in a petri dish, a process called culture, and can take between three days and one week; and a much faster molecular testing through the GenXpert.
Testing for TB after medication is crucial to confirm the eradication of the bacteria and ensure the success of treatment. This testing helps prevent the spread of TB, identifies potential treatment failures or drug resistance, and confirms that the individual is no longer contagious. If the tests show persistent or returning TB bacteria, it could mean treatment failure or the emergence of drug-resistant strains, necessitating adjustments to the treatment plan.
TB mimicking other diseases
Dr. Andrew Owuor, a lung specialist at Kenyatta National Hospital (KNH), said that testing is a do-or-die step for people.
“TB can mimic many other diseases, and the only way to give the appropriate medication is after confirming whether they have TB,” Dr. Owuor told Defrontera.
Working at KNH—the biggest health facility in Kenya and the East African region—Dr. Owuor says he sees “regular TB patients” because “the physicians at the primary health facilities can often diagnose and institute treatment.” The cases he sees are from normal.
“I see complications that arise from TB... people who are coughing blood, can barely walk, and have severely damaged lungs, all from pulmonary TB, the infectious type of TB… there are other types of TB that affect all parts of the body… bones, skin… the only parts of the body TB does not affect are hair and teeth,” says Dr. Owuor.
Testing is critical because the bacterium that causes TB—Mycobacterium tuberculosis—can sometimes lie dormant in the human body for decades, an infection called latent tuberculosis infection. The WHO states that one in every four people in any population has latent TB, and when an opportunity arises—such as when the immune system is suppressed, as is common in HIV patients—the bacterium activates, making that person sick and quickly transmitting the disease to others.
A TB patient not on medication is particularly dangerous for counties like Siaya. There are more than 93,000 people living with HIV in the county, among the top five of the 47 counties in Kenya, according to the latest estimates from the National Syndemic Diseases Control Council (NSDCC). People living with HIV are 29 times more likely to develop TB disease compared with people without HIV.
Siaya County’s Executive Committee Member (CECM) for Health, Dr. Martin Odhiambo K’Onyango, told Defrontera on the phone that the county, like the rest of the country, has been affected by the USAID stop work order (we have reported on the Stop Work Order) and—like the rest of the world—waits for the main decision from the Trump Administration in coming days.
“We have been impacted by the USAID stop work order and we are still feeling the impacts to date. We do not have the same number of people as before. Service delivery logistics has also been affected,” he said without giving specifics on the number of people the county had to let go.
On TB drug stockouts, Dr. Odhiambo said the county has been facing shortages of two paediatric drugs—Rifampicin and Isoniazid—for more than two years now due to supply-related issues. The two drugs prevent children from becoming ill from the active form of TB. The bacteria that cause TB are hard to kill, and infected children are more likely to develop TB disease than infected adults and are also more likely to become seriously unwell.
“After the stop work order, service delivery for TB has been affected by between 20 and 30 percent,” he said.
Despite taking the medication as prescribed this second time round, Joel says he feels worse, always tired and out of breath, with constant body aches. He eats regularly, but he sees his body fading off, so much so that he can see his two nieces, the ones he lives with, often cry as they watch him take his medication.
"People take drugs to get better, but I have not seen any change and now I sometimes see my children crying while I take my medication," he adds.
Just by looking at Joel, Elizabeth Achieng' Onyango—a community health promoter who visit him from time to time to ensure he takes his medication—has a plausible explanation for Joel’s gaunt physique and deteriorating health.
“He may not have taken his medication daily despite his insistence that he did, or he has drug-resistant TB,” Elizabeth told Defrontera.
Community health promoters like Elizabeth are part of the health system in Kenya and they visit households to carry out health education, and check that children have been vaccinated, among other tasks.

Elizabeth’s job includes ensuring that those living with HIV and Tuberculosis adhere to their medication schedule. Joel’s is one of the 144 homes (about 600 people) that Elizabeth visits in Ralak and Krindo villages in Ugunja Subcounty in Siaya County.
Elizabeth says she is not sure whether Joel has chosen not to visit the clinic for testing, or the lower-level health facility in Simenya did not write him a referral letter. In some instances, the 52-year-old has said that he is too weak to visit Ambira Hospital and in others he does not have KES 200 (about $1.5) for fare.
22,000 coughs
Despite the potential of being sickly, Joel continues to mingle with his community and friends daily, oblivious to how contagious the disease is. Joel, who worked in the public transport sector, still has friends, including drivers and conductors, in the industry he meets regularly at local entertainment joints in Simenya. He also lives with his sister's child, who assists him when overwhelmed. Yet, a person with active TB and not on treatment can potentially infect as many as 15 other people within a year through close contact.
Lung specialists worry about a suspected TB case walking around, mingling with other members of the community because of how TB spreads. For a long time, it was believed that people with TB transmitted it to others when the infected individual coughed and sprayed droplets containing the bacteria into the air.
But in 2021 research, researchers from the University of Cape Town in South Africa found that an infected person breathes about 22,000 times per day and only coughs about 500 times. The researchers called this tidal breathing: when a person inhales, their air sacs in the lungs open and when they exhale, the bacteria move from the lungs via aerosols.
If Joel has TB and he is not on treatment, his very existence and mere act of breathing in the local drinking joints that he visits with his friends spread the disease to those around him.
Now, more than ever, the health system cannot afford to have potential TB patients in the community without treatment, as the funding for diagnosing and treatment of TB remains in a limbo with funding cuts from the United States. In its 2023 annual report, the National Tuberculosis, Leprosy and Lung Disease Programme (NTLDP) reported that the country had only raised KES 2.7 billion against the required KES 7.22 billion—over 60% funding gap. The report noted the funding sources included the Government of Kenya (10%), the Global Fund (64%), USAID (25%) and CHAI (1%).”
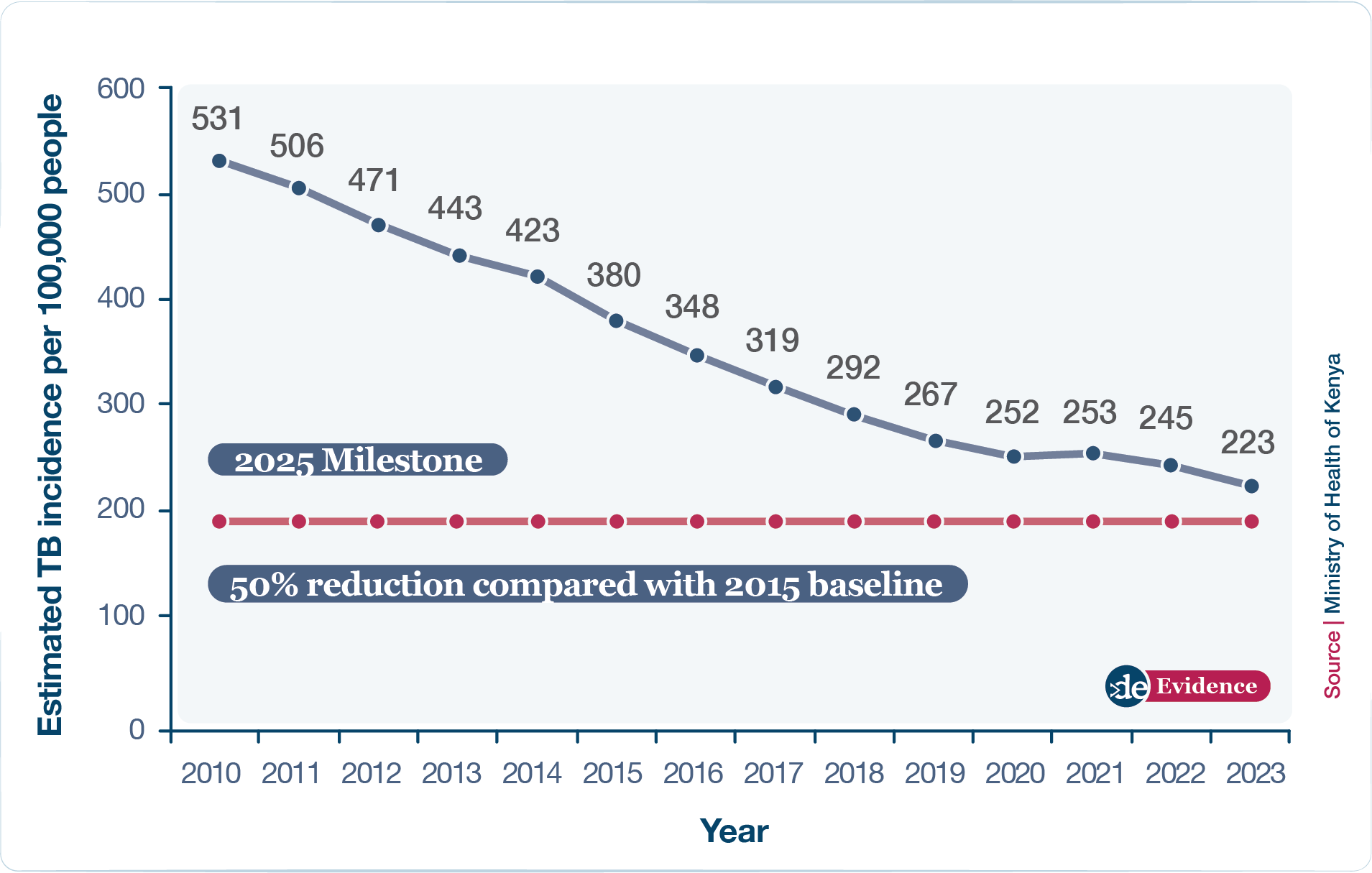
The gap in funding puts patients like Joel at risk. Such patients, even if they do not need drugs, would need tests and follow-ups. Already, Kenya's healthcare system is dealing with shortages of the first line of anti-TB drugs, which is threatening to reverse gains made in curbing new TB infections. Health workers who spoke to Defrontera from five counties—Kajiado, Nairobi, Nakuru, Bungoma, and Kakamega—say the shortages started late last year and grew to late March this year, even as the country prepares to face a new TB funding crisis from President Trump's USAID cuts.
A healthcare worker in Kakamega County in western Kenya who did not want to be named for fear of being victimised told Defrontera that he has turned patients away untreated whenever the county faced shortages. He said the shortages were worse between December and February this year, but supply has now stabilised. He said that stockouts for drugs given to patients when they are exposed to TB to prevent infections, and the medication for treatment, is a serious cause of concern as the bacterium that causes TB easily mutates when exposed to low drug pressure. This, in turn, causes multi-drug resistance (MDR), producing more potent and virulent bacteria, resulting in harder-to-treat TB infections.
"Clients cannot, therefore, be initiated on TB prophylaxis or treatment because there is not enough stock to go all the way to completion, bearing in mind that it is not recommended to interrupt treatment once initiated due to the risk of MDR," he told Defrontera.
In dire cases, some patients are forced to share drug packs, and this leads to adverse health outcomes for patients who must travel long distances to get drugs. Some counties have also had to redistribute available stock in the short term.
Sources within the Kenya Medical Supplies Authority (KEMSA), the government agency tasked with distributing drugs, and who requested not to be named for fear of victimization confirmed that the shortage was made severe due to huge pending bills from counties that have made it difficult for the agency to supply new stocks to the facilities. Contacted for an official comment, KEMSA referred Defrontera to the NTLDP, which deals with the disease. Despite the concerns that some counties have reported, the NTLDP maintained that TB drugs are available and distributed to all counties.
This story is part of Gasping for Breath, a special focus on Tuberculosis.
Share this feature

